
ACL Answers from a Vail KNEE DOCTOR: ACL Injuries, Surgery and Options

Hey Dr S, just wondering what the correct "timing" is to have my ACL fixed. Thanks!
The right time to have an ACL operation is when the knee is ready to handle the intensive rehabilitation required afterwards. We have presented a study looking at the risk of developing scar tissue enough to require more surgery.
When the knee has limited swelling, 0-120 degrees of motion and can do a straight leg raise without a lag it is ready for surgery. This may take 1 day or 1 month to “get ready”.
Here's what's need before you undergo ACL Surgery:
- 0-120 degrees ROM
- Limited Swelling
- Straight Leg Raise without a lag
The good news is that we now have methods of getting most everybody back to their chosen lifestyle following an injury to the dreaded Anterior Cruciate Ligament.
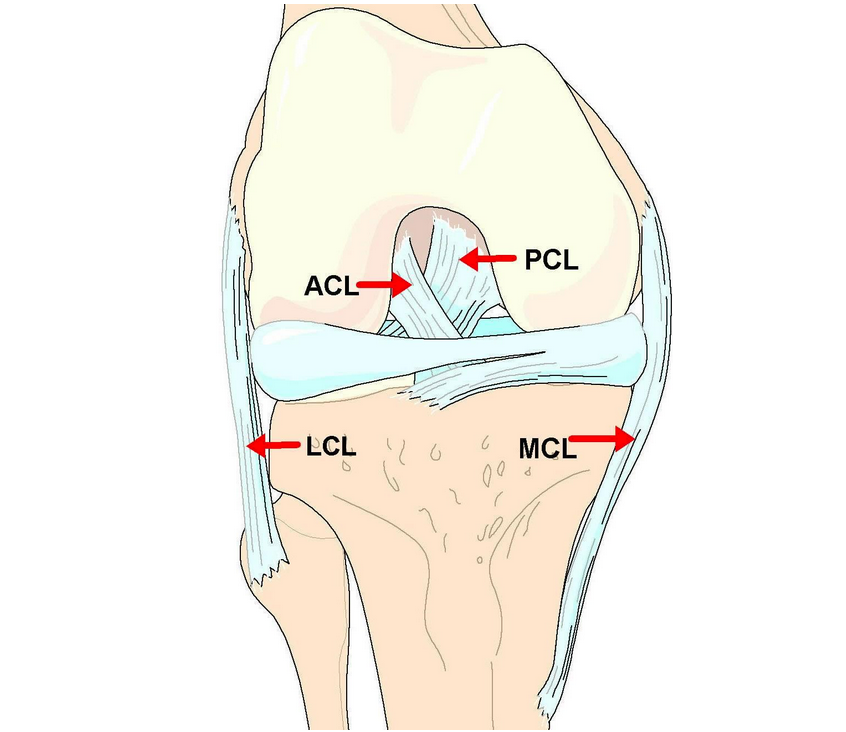
This diagram features the knee ligaments. Note the ACL (Anterior Cruciate Ligament).
Patellar Tendon or Hamstring?
“Our options for replacing the ACL include a cadaver graft, your own patellar tendon or hamstrings. All are very strong, in fact stronger than a native ACL in most circumstances. ”
Unfortunately, not only will the ACL not heal on its own, sewing the ACL only seems to work about 65% of the time. Replacing the ACL works 98% of the time. Therefore the most common surgical procedure on the ACL is replacement or “reconstruction”.
Our options for replacing the ACL include a cadaver graft, your own patellar tendon or hamstrings. All are very strong, in fact stronger than a native ACL in most circumstances.
To replace the ACL we must make tunnels in the bone to place the new graft. The patellar tendon graft has bone plugs on either end and has the advantage of bone-to-bone healing. which typically occurs in 4 weeks.
The hamstring graft is all soft tissue and takes 8-12 weeks to incorporate into the bony tunnels. Both grafts will go through a process of weakening followed by revascularization, and won’t achieve maximum strength until about 9 months after surgery.
Patellar Tendon Graft with a Bone Plug on Either End
For the young, high level athlete we tend to favor the Patellar Tendon Reconstruction due to the lower re-rupture rate we have found.
In the high-level recreational athlete who needs to get back to work as soon as possible, we would often favor the Hamstring Reconstruction.
Both graft choices are extremely strong and work exceptionally well with the proper rehabilitation.
What's the deal with Knee Ligaments?
Ligaments seem to confuse the heck out of everybody although understanding them can actually be quite easy. A ligament is a tight band of tissue that connects a bone to a bone, and crosses a joint. It doesn’t stretch, contract or move. Just by virtue of where it is located, it provides stability against a particular motion to that joint.
“The ACL, therefore, is only in our knee to protect the meniscus; the meniscus is only there to protect the articular cartilage. Once the articular cartilage is gone, we have “arthritis” which is just the phenomenon of bone rubbing on bone. ”
There are 4 ligaments about the knee we talk about. The most commonly injured in skiing is the MCL, on the inner side. This is a "good" ligament to hurt because it will typically heal on its own with the proper bracing and rehabilitation. The duration it takes the MCL to heal is dependent upon how severe the tear is, partial or complete.
The one we hear so much about in sports is the “ACL”, or Anterior (front) Cruciate (crossing) Ligament. We test this by pulling the leg forward of the thigh, but the ACL’s function is mostly in preventing twisting injuries to the knee.
Without the ACL we place a lot of shear strain on the meniscus, or cushion cartilage. When this gets worn down too much we are left with the articular cartilage only.
The ACL, therefore, is only in our knee to protect the meniscus; the meniscus is only there to protect the articular cartilage. Once the articular cartilage is gone, we have “arthritis” which is just the phenomenon of bone rubbing on bone.
What Happens When the ACL is Torn?

Unlike the MCL, the ACL typically does not heal on its own. However loose a knee is after the ACL is torn, is how loose it will be 1 year, or 5 years down the line.
“ACL deficient athletes had more than a 20 x increased risk of sustaining a knee injury requiring surgery than skiers with normal knees in this skiing population!”
Let's reference a recent study, looking at professional skiers at Vail (mostly Ski Instructors and Patrol) who were skiing without an ACL. ACL deficient athletes had more than a 20 x increased risk of sustaining a knee injury requiring surgery than skiers with normal knees in this skiing population!
Once you have torn your ACL, you have three options:
You can live without an ACL and modify your activities so that you are not at increased risk.
You could live without an ACL, not modify your activities, and recognize that you are at increased risk for a significant knee injury
You could have your ACL fixed.
There is no one right answer for everybody, but being realistic about your lifestyle and expectations will usually lead us to the right decision for you.
What are some optios for non-Operative Treatment of the ACL Deficient Knee?

“Not wearing a brace led to a more than 6 fold increased injury risk within the population of ACL deficient skiers. ”
The two ways of protecting the internal structures of the knee are the ligaments and the muscles. Ligaments provide the majority of our protection from twisting injuries. Once the ACL is gone we rely on the muscular anatomy that much more.
The quadriceps and hamstrings play a vital role in protecting our joint. Other adaptive mechanisms include absorbing more of the energy of landing with the ankle and should be taken into account when devising a non-operative rehabilitation strengthening program.
We have recently completed a study of Vail Resorts Ski Instructors who were ACL Deficient and broke them into those that were wearing an ACL brace versus those that weren’t. Not wearing a brace led to a more than 6 fold increased injury risk within the population of ACL deficient skiers.
Maintaining good conditioning of the quadriceps and hamstrings, avoiding twisting sports and ACL bracewear during sports at risk are the best techniques available in a non-operative fashion to the ACL Deficient athlete for injury prevention.











